Technical Notes: HIV exposure categories
An attempt is made to assign each HIV test to an exposure category based on what reported HIV risk factor information is collected on the requisition form. The exposure category is meant to represent an individual’s most likely means of HIV acquisition. The exposure categories are mutually exclusive. When more than one risk factor is reported for a single individual, a hierarchy is used to assign an HIV test to a single exposure category.
This hierarchy is as follows:
- Mother-to-child transmission (MTC): Being a child of an HIV-positive mother or aged less than 18 months
- Male-to-male sexual contact + injection drug use (IDU): Being male and indicating sex with men and injection drug use
- Male-to-male sexual contact: Being male and indicating sex with men
- Injection drug use (IDU): Indicating injection drug use
- HIV-endemic
- HIV-endemic + heterosexual contact: (Country of birth is HIV-endemic or “Born in an HIV-endemic country” indicated as HIV risk factor) + indication of heterosexual contact (defined as being male or female and indicating sex with a person of the opposite sex/gender)
- HIV-endemic, no heterosexual contact: (Country of birth is HIV-endemic or “Born in an HIV-endemic country” indicated as HIV risk factor) + no indication of heterosexual contact as in 5a
- Heterosexual contact – partner with identified risk (PIR): Being male or female and indicating sex with a person of the opposite sex/gender who is either HIV-positive, uses injection drugs, born in an HIV-endemic country, or is a bisexual male.
- Heterosexual contact, no identified risk: Being male or female and indicating sex with a person of the opposite sex/gender who has no identified risk.
- Clotting factor (pre-1986): Indicating clotting factor pre-1986
- Transfusion (pre-1986): Indicating a blood transfusion pre-1986
- No identified risk (NIR): Indicating “none” or “other” or “needlestick injury” as a risk factor
Starting with the report « HIV diagnoses in Ontario, 2019 » and in future reports, OHESI combines some of the above categories to form broader categories as such:
- Heterosexual contact, identified risk: combines diagnoses assigned to “HIV-endemic + heterosexual contact” (category #5-1 above) and “Heterosexual contact – partner with identified risk (PIR)” (category #6)
- Other: combines diagnoses assigned to “Mother-to-child transmission (MTC)” (category #1), “Clotting factor (pre-1986)” (category #8), and transfusion categories (category #9).
- No risk reported/unknown: combines diagnoses assigned to “HIV-endemic, no heterosexual contact” (category #5-2) and “No identified risk” (category #10), or where the form is not completed (category #11).
HIV-endemic areas (category #5) are classified by the Public Health Agency of Canada as countries where the prevalence of HIV among adults (15-49 years old) is 1.0% or greater and one of the following criteria is met: at least 50% are attributed to heterosexual transmission; a male to female ratio of 2:1 or less among prevalent infections; or HIV prevalence greater than or equal to 2% among women receiving prenatal care. A list of these countries can be found here.
HIV risk factor data used to determine an individual’s exposure category is missing for about one quarter of first-time HIV diagnoses (average of 24.4% per year between 2015 and 2019). These tests are included in figures of numbers of diagnoses and excluded from figures of proportions by HIV exposure category.
It is unknown whether individuals with certain HIV risk factors, and hence exposure categories, are more likely to be missing information, which could introduce bias into the exposure category breakdowns. Also, provider practices for filling out the requisition forms may vary, leading to further bias. For example, some providers may ask people getting tested about their risk factors, while others may make assumptions or not ask.
In 2018, a “country of birth” field was added to the HIV test requisition form which better informed attribution to the HIV-endemic exposure category and likely contributed to the larger proportion of HIV tests attributed to this category in this year and 2019. As exposure category attribution follows a hierarchy, increasing proportions in higher categories would decrease proportions attributed to subsequent categories. Any interpretation of changes between exposure category proportions of HIV tests in 2018 or 2019 and the years prior should remain mindful of this caveat.
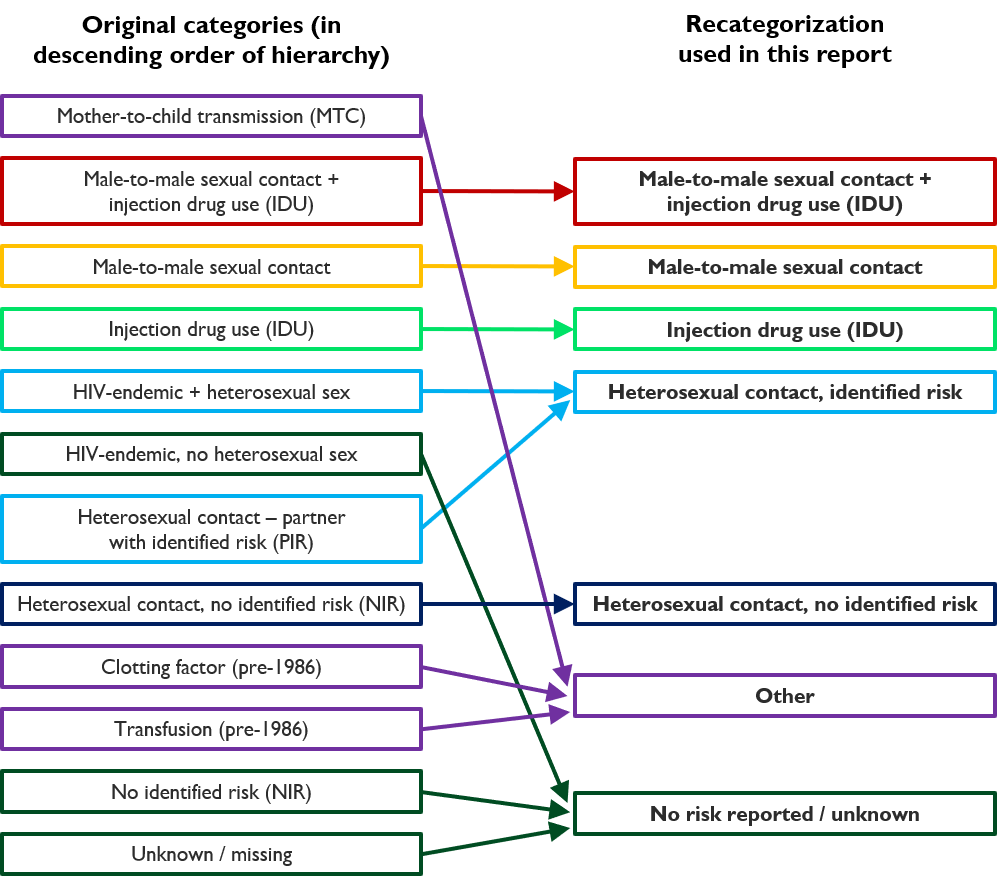
Figure i: Original hierarchical HIV exposure categories (in descending order) and how they are recategorized.